FR | EN
The role of the menstrual cycle in embryo implantation
From puberty to menopause, the menstrual cycle is a physiological mechanism that prepares a woman's body for a possible pregnancy, and therefore for possible embryo implantation. With an average duration of 28 days, each menstrual cycle can last from 21 to 35 days. During each cycle, the uterine lining, known as the endometrium, undergoes cyclical renewal, alternating between phases of regression, proliferation, and maturation. These different phases are influenced by hormones produced by the ovaries: oestrogen and progesterone.
The menstrual phase
The first day of menstruation initiates the menstrual phase. Lasting three to six days, it corresponds to the destruction of the endometrium. In the absence of an embryo in the uterine cavity, the corpus luteum regresses in the ovary: progesterone production falls sharply. This drop in hormone levels leads to thinning and atrophy of the endometrium.
The proliferative phase
The proliferative or regenerative phase begins on the last day of menstruation (menstruation) and ends with ovulation. It takes place under the action of oestrogens produced by the growing ovarian follicles. The increase in oestrogen levels leads to the proliferation of endometrial cells, causing them to thicken. At the end of this phase, the uterine mucosa reaches a thickness of 10 to 12 millimetres.
The secretory phase of the menstrual cycle
The secretory phase begins at ovulation and continues until the end of the cycle. In the ovary, the follicle that released the oocyte during ovulation is transformed into the corpus luteum. This produces increasing quantities of progesterone, which leads to the differentiation of the endometrial glands. These will produce molecules that are essential for the survival of the embryo in the early stages of pregnancy (nutrient molecules, immune molecules, adhesion molecules). During the secretory phase, the embryo is implanted.
The receptive endometrium and embryo implantation
Embryo implantation requires a synchronous dialogue between a competent embryo (blastocyst stage) and a receptive endometrium. This period of endometrial receptivity to the embryo is called the implantation window. The implantation window corresponds to the period during which the endometrium is ready to receive an embryo. It occurs between days 7 and 11 following ovulation or puncture. Outside this window, the endometrium is completely resistant to implantation.
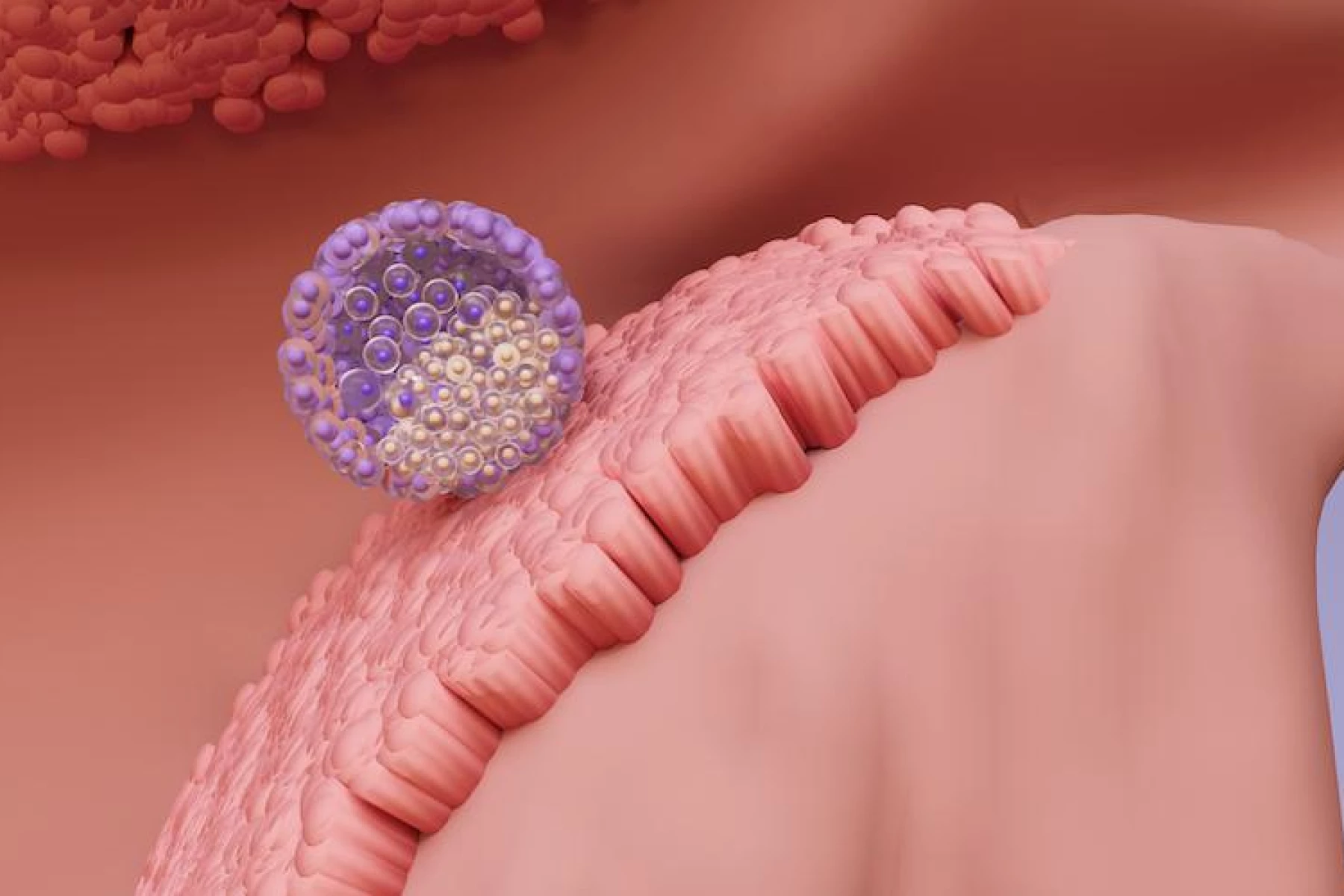
The embryo implantation process
Embryo implantation is a multi-stage process. It begins with the opposition of the embryo to the endometrium. Next, the embryonic cells and the endometrial cells of the uterus establish close molecular contact: this is adhesion. Finally, the trophoblastic cells multiply intensely and allow the embryo to invade the endometrium. The embryo then buries itself completely in the uterine mucosa during implantation.
How do I know if the embryo has been implanted?
Following implantation, the embryonic cells continue to multiply. These cells are responsible for the formation of the placenta, which produces the main pregnancy hormones. Among these hormones, ß-hCG is synthesised very soon after embryonic implantation. A high and rapidly changing level of ß-hCG in the blood is a sign that the early stages of pregnancy are proceeding normally.
ß-hCG levels in the blood are a sign of successful embryo implantation
Ideally, the concentration of this hormone in the blood should be measured around ten days after the transfer (on the presumed date of the next menstrual period). This is done by taking a blood sample. A result of more than 50 mIU/ml is a sign of pregnancy.
One month after the transfer, an ultrasound examination confirms the presence of an embryo within the uterine mucosa. It should be borne in mind, however, that miscarriages are common during the first trimester. However, at this stage, a pregnancy resulting from medically assisted procreation has the same chances of reaching term as a spontaneous pregnancy.
However, the chances of embryo implantation and pregnancy remain unpredictable. Failures can be linked to both the quality of the embryo (chromosomal anomalies, damaged DNA, etc.) and the quality of the endometrium (uterine malformations, lack of receptivity, inflammation, etc.). In medically assisted procreation, the implantation rate is 25% for embryos transferred at the 8-cell stage. This rises to 30% when the embryo is transferred at the blastocyst stage.


